What exactly is Obstructive Sleep Apnea (OSA)?
Obstructive Sleep Apnea (OSA) is a serious sleep disorder where your breathing repeatedly stops and starts throughout the night.
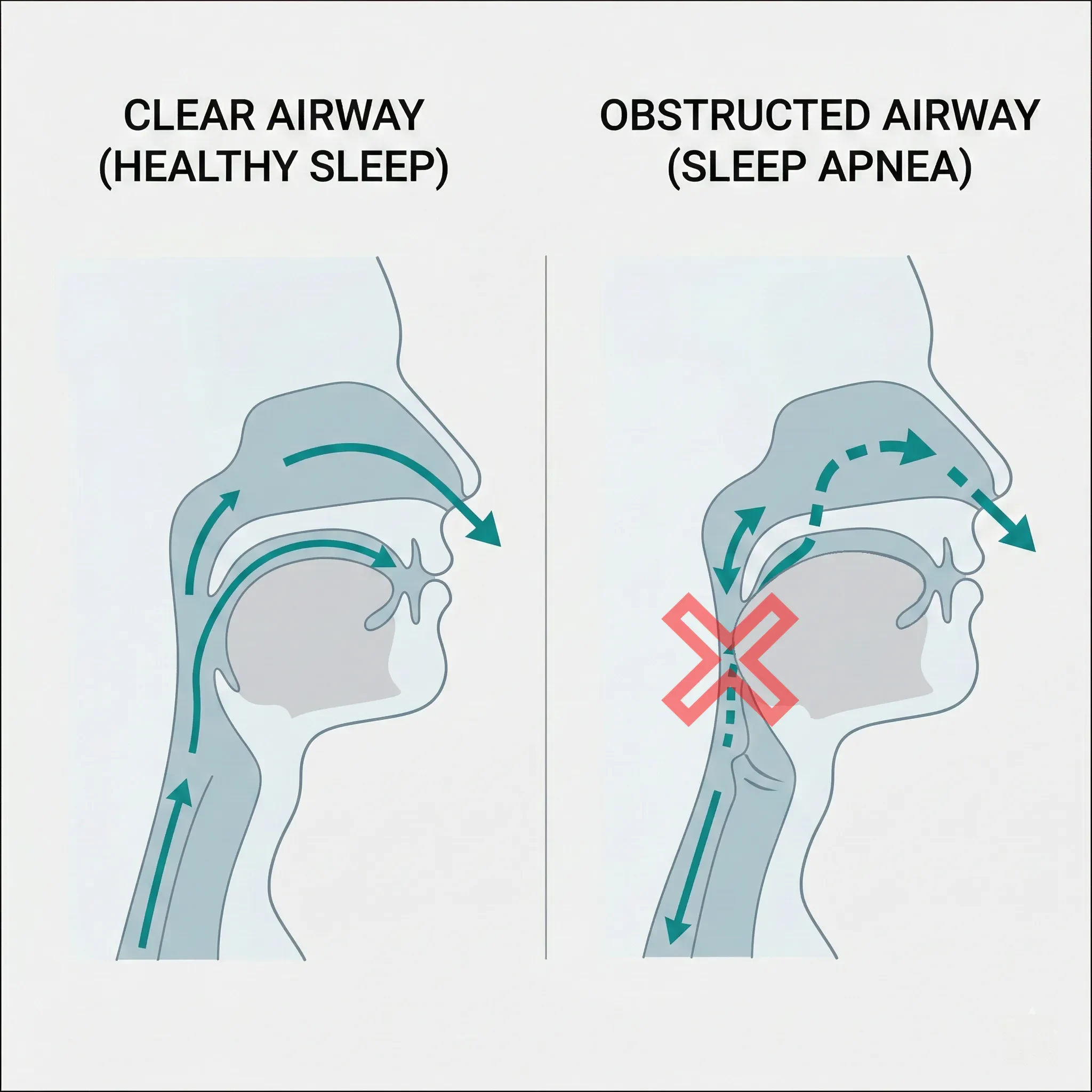
It occurs when the muscles in the back of your throat physically relax. When these muscles relax, the soft tissues—including your tongue and soft palate—can collapse into the airway, creating a physical blockage that restricts or completely cuts off airflow to your lungs.
This is not just snoring. Snoring is caused by tissue vibrating as air squeezes past, but an “apnea” (an obstruction) means you have temporarily stopped breathing. When this happens, your blood oxygen levels drop, and your brain must partially wake you up to force your muscles to reopen the airway, leading to severely fragmented, non-restorative sleep.
What are the most common warning signs?
Sleep apnea often goes undiagnosed because the most significant symptoms happen while you are unconscious. However, the “daytime hangover” and certain nighttime behaviors are major red flags.
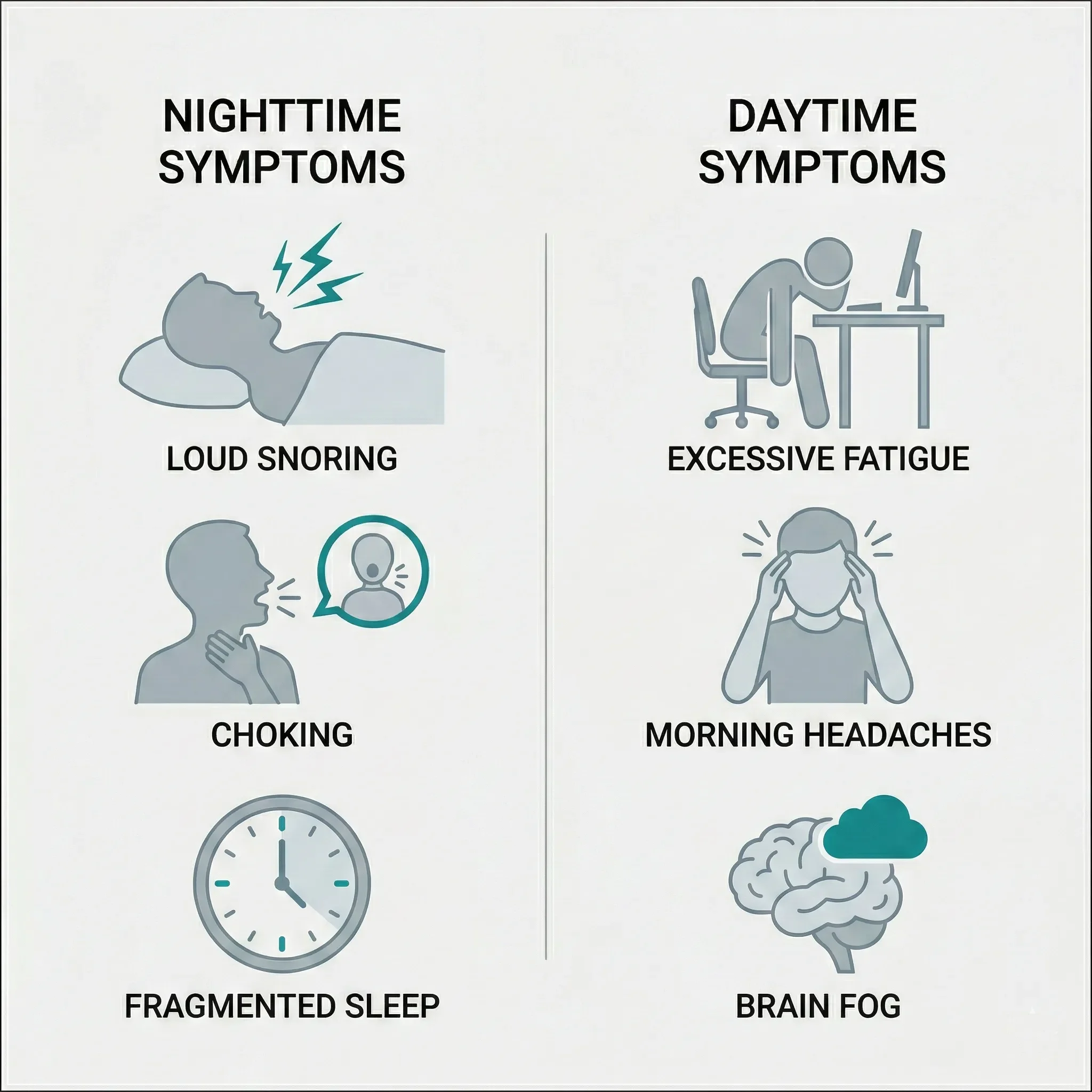
Common Nighttime Symptoms:
- Loud, Persistent Snoring: Especially snoring that is interrupted by silences (pauses in breathing).
- Gasping or Choking: Waking up suddenly feeling like you are catching your breath.
- Restless Sleep: Frequent tossing and turning or waking up to use the bathroom multiple times a night (Nocturia).
Common Daytime Symptoms:
Dry Mouth: Waking up with a very dry or sore throat from open-mouth breathing and snoring.
Excessive Daytime Sleepiness: Feeling like you could fall asleep at your desk, during a movie, or while driving.
Morning Headaches: Caused by the lack of oxygen and the widening of blood vessels in the brain during the night.
“Brain Fog”: Difficulty concentrating, memory lapses, or feeling irritable and moody.
Is snoring always a sign of sleep apnea?
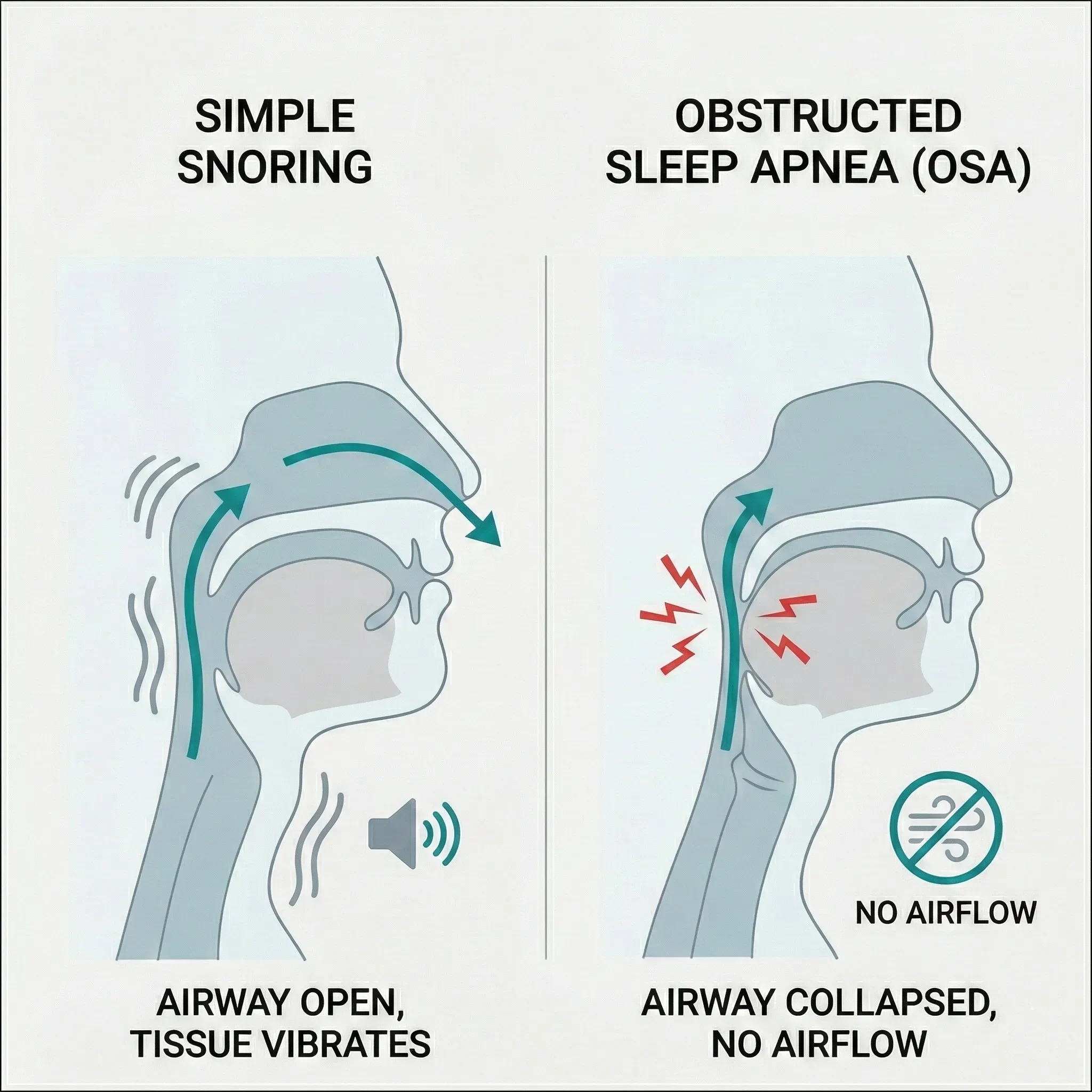
Not everyone who snores has sleep apnea, but almost everyone with obstructive sleep apnea snores.
“Simple Snoring” occurs when the airway is partially narrowed, causing tissues to vibrate. While it can be disruptive to a partner, it doesn’t necessarily stop your breathing or drop your oxygen levels.
Sleep Apnea is different because the airway doesn’t just narrow—it closes. If your snoring is accompanied by gasping, daytime fatigue, or high blood pressure, it is likely more than “just snoring” and should be screened immediately.
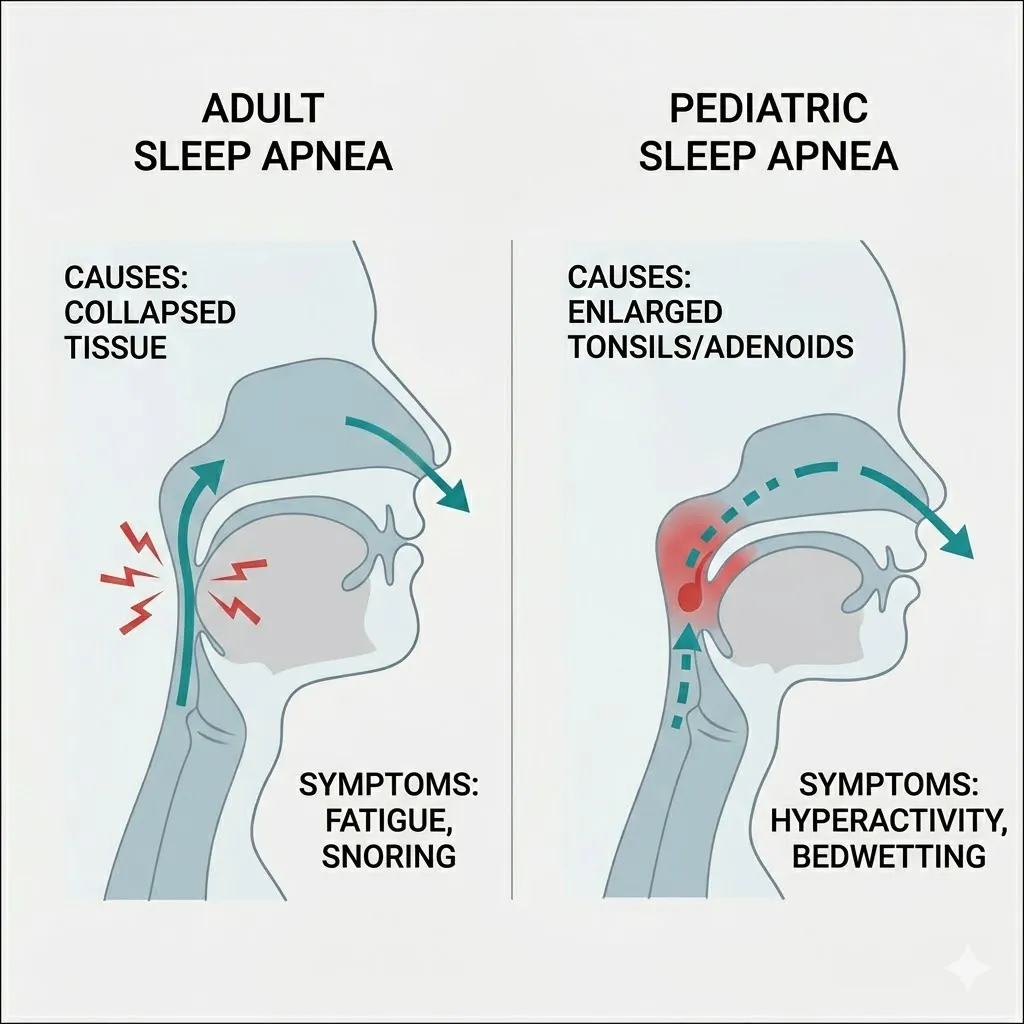
Can children have sleep apnea?
Yes, though it often looks different in children than it does in adults. While adults tend to become sluggish and sleepy, children with sleep apnea may become hyperactive.
Because their brains are struggling to stay awake, they may exhibit behaviors that mimic ADHD, such as:
- Difficulty paying attention in school.
- Aggressive or irritable behavior.
- Bedwetting.
- Sleeping in unusual positions (e.g., with their neck arched far back).
In children, sleep apnea is frequently caused by enlarged tonsils or adenoids, and a consultation with a pediatrician is the vital first step.
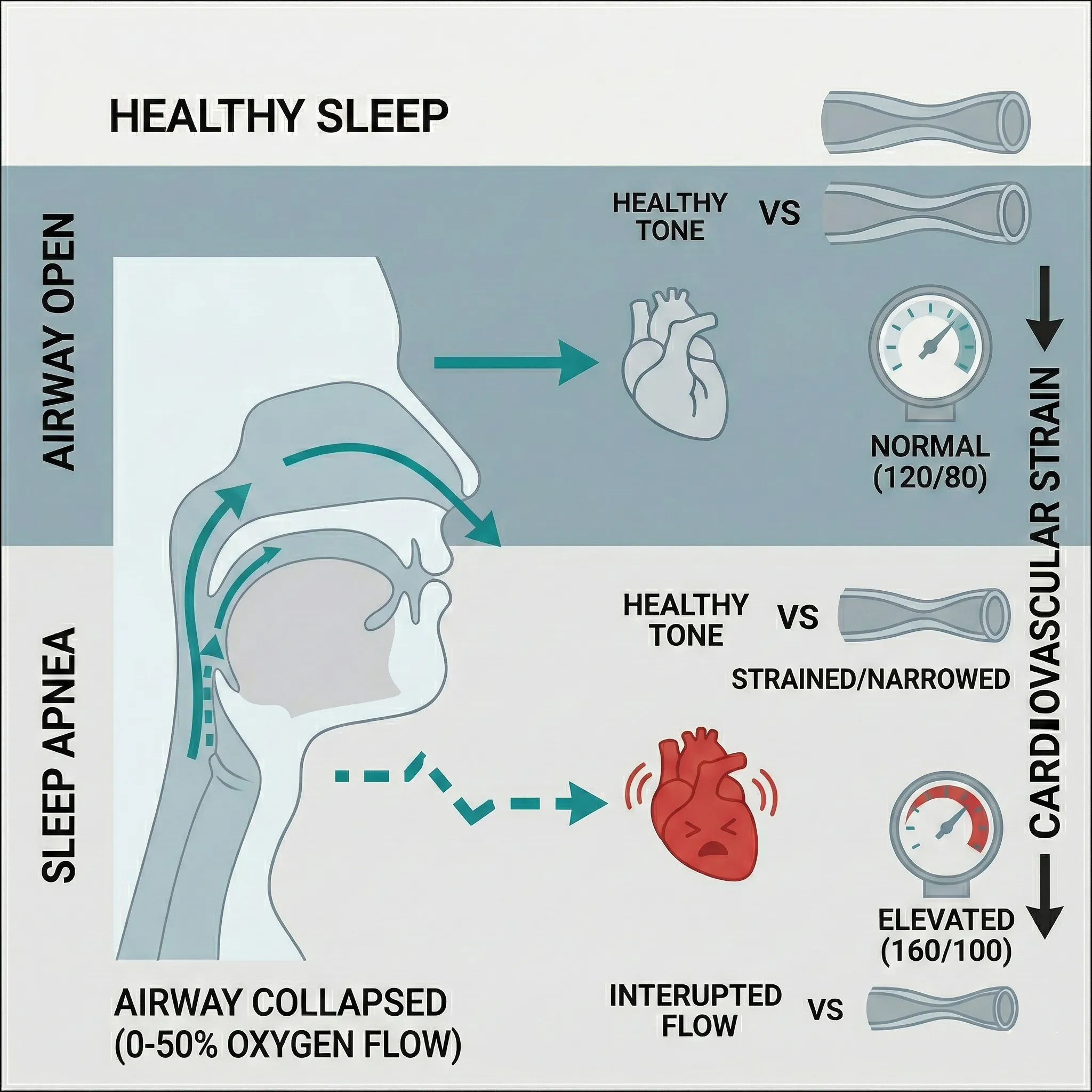
How does sleep apnea affect my heart?
Sleep apnea and heart health are deeply connected. Every time your breathing stops, your blood oxygen levels plummet. In response, your brain releases a surge of adrenaline and stress hormones (cortisol) to wake you up and restart your breathing.
This repeated “fight or flight” response causes your heart to beat faster and your blood pressure to spike. Over months and years, this constant nighttime strain leads to:
Heart Failure: The heart becomes overworked and less efficient at pumping blood.
Hypertension (High Blood Pressure): Your body stays in a state of high pressure even during the day.
Atrial Fibrillation (Afib): The physical strain on the heart’s chambers can trigger irregular heart rhythms.
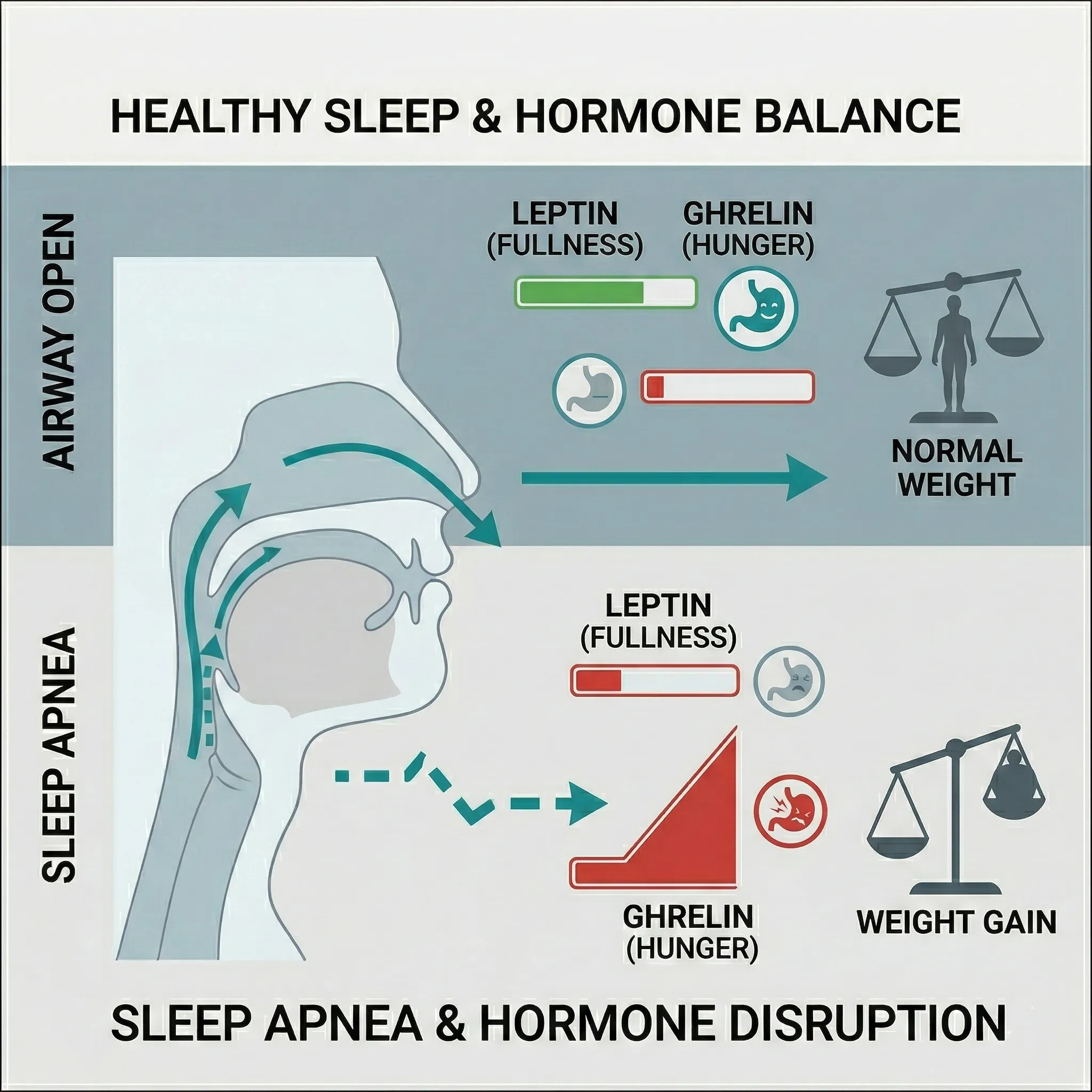
Can sleep apnea cause weight gain?
Yes, and it often creates a “vicious cycle.” While excess weight is a risk factor for sleep apnea, sleep apnea itself makes it much harder to lose weight due to hormonal disruption.
When you don’t get deep, restorative sleep, your body mismanages two key hunger hormones:
- Ghrelin Increases: The “hunger hormone” goes up, making you crave high-calorie, sugary foods for quick energy.
- Leptin Decreases: The “fullness hormone” goes down, so your brain doesn’t receive the signal that you are satisfied after eating.
Furthermore, the extreme fatigue caused by apnea makes it difficult to find the energy for physical activity, leading to further weight gain which, in turn, worsens the airway obstruction.
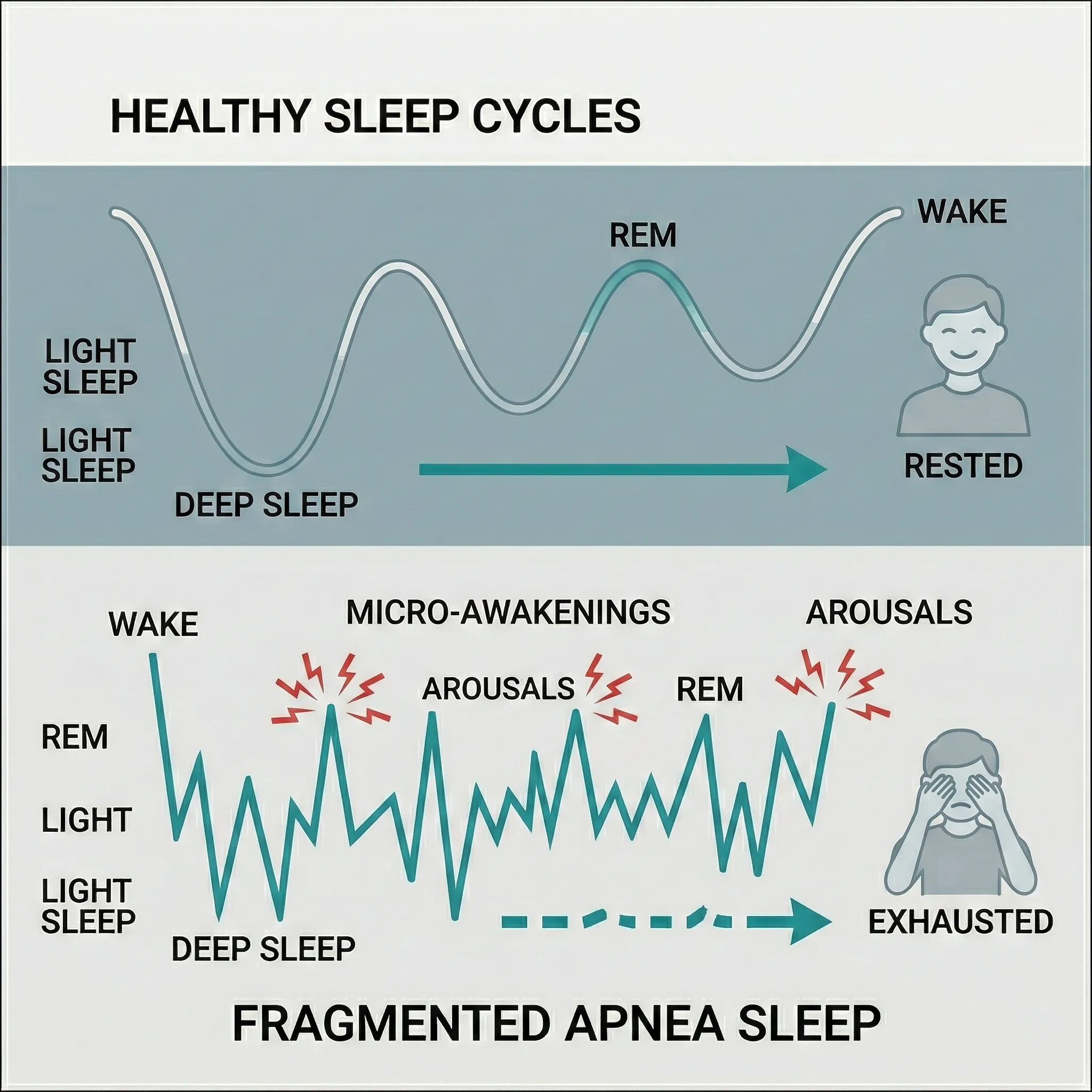
Why am I so tired even after 8 hours of sleep?
It isn’t about the quantity of sleep; it’s about the quality. You may be in bed for 8 hours, but if you have sleep apnea, you are likely suffering from hundreds of “micro-awakenings” that you don’t even remember.
These awakenings prevent you from entering and staying in the two most important stages of sleep:
- Deep Sleep (Slow Wave Sleep): Crucial for physical repair and immune function.
- REM Sleep: Essential for memory consolidation and emotional regulation.
Because your brain is constantly “jolted” awake to breathe, you spend the entire night in light sleep. This is why you wake up feeling unrefreshed, often described as a “sleep hangover.”
How do I get a formal diagnosis?
Getting a diagnosis is the most important step in treating sleep apnea. Traditionally, this required an overnight stay at a hospital “sleep lab,” but today, most people can be diagnosed from the comfort of their own bed.
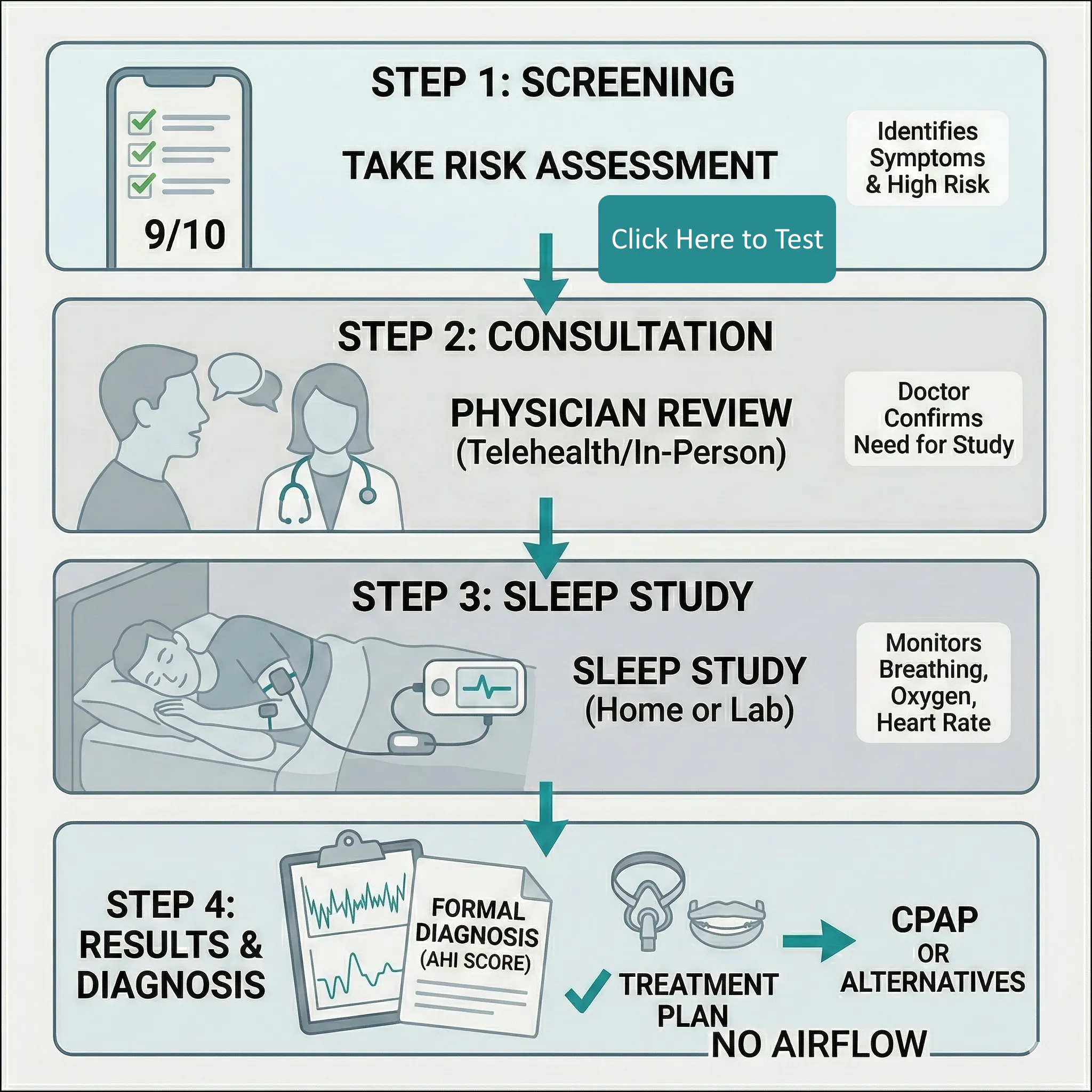
The process generally follows these steps:
Review: A board-certified sleep physician reviews the data and provides a formal diagnosis and treatment plan.
Screening: Using a tool like our Apnea Risk Score to see if your symptoms warrant a clinical test.
Consultation: Speaking with a physician (in-person or via telehealth) to review your history.
The Sleep Study: Monitoring your breathing, heart rate, and oxygen levels for at least one night.
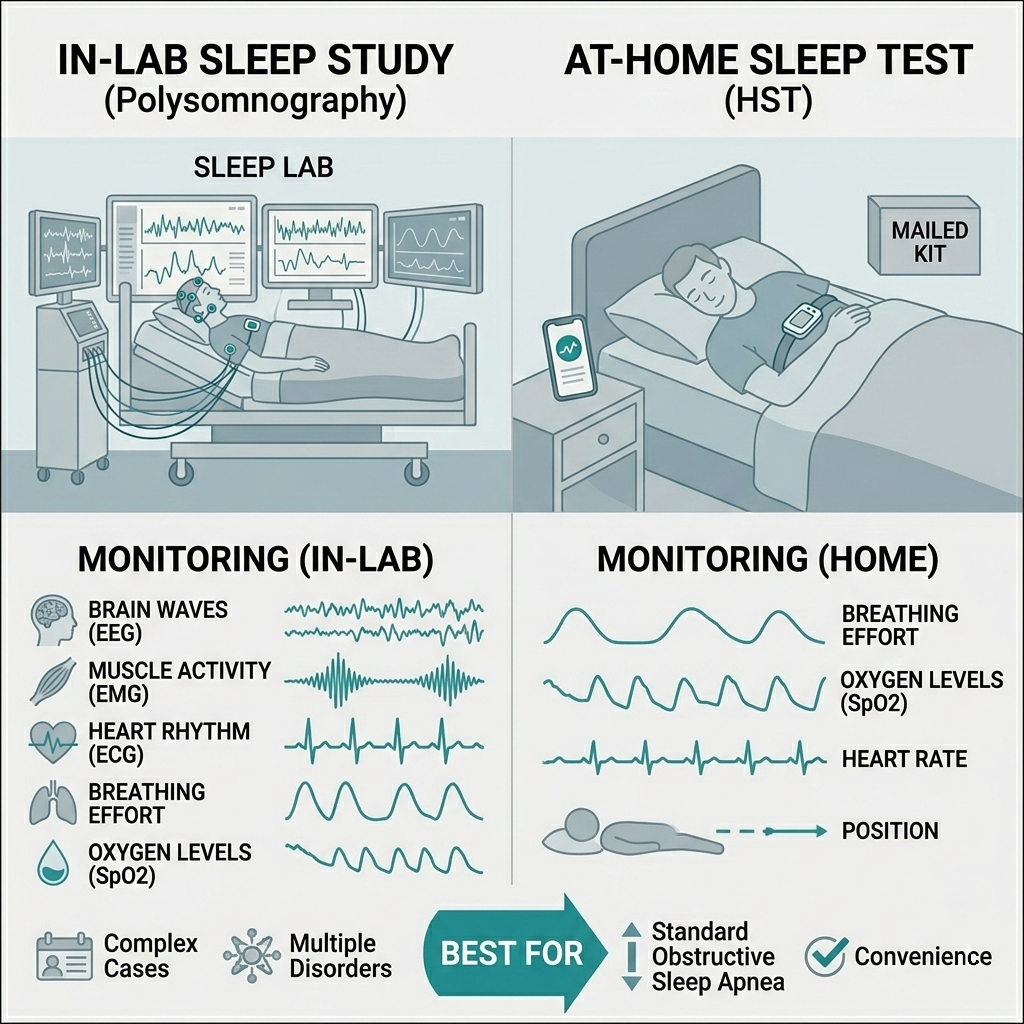
What is the difference between an In-Lab and At-Home Sleep Test?
The “Gold Standard” depends on your specific health needs:
At-Home Sleep Test (HST): You receive a small, portable device in the mail. You wear it for one night at home and ship it back (or upload the data). It is much more comfortable, significantly cheaper, and highly effective for diagnosing standard Obstructive Sleep Apnea.
In-Lab Study (Polysomnography): You sleep in a specialized clinic while connected to various sensors. It monitors brain waves, muscle activity, and heart rhythm. This is usually required for complex cases or if the doctor suspects other sleep disorders like narcolepsy.
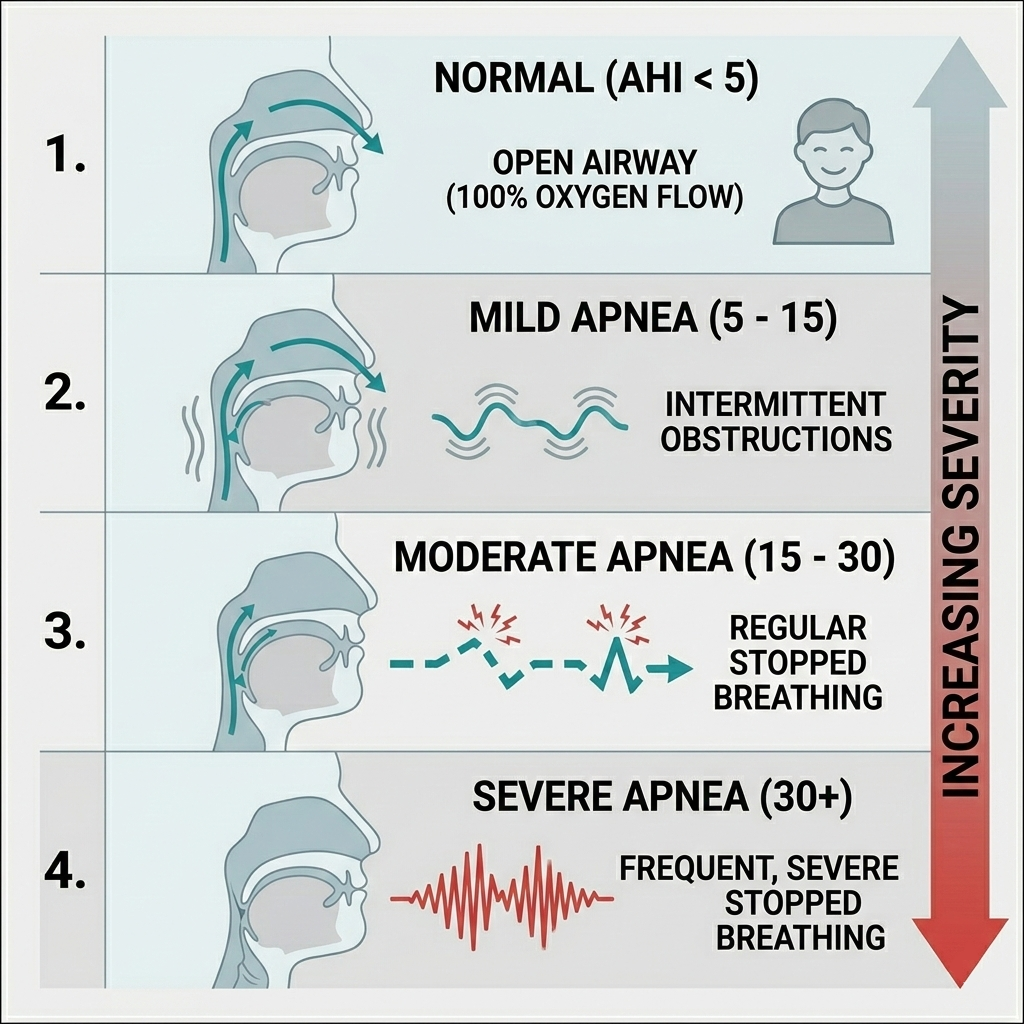
What is an AHI score?
When you receive your results, the most important number you will see is your AHI (Apnea-Hypopnea Index). This number represents the average number of times your breathing stopped (apnea) or became shallow (hypopnea) per hour of sleep.
The Severity Scale:
- Severe Sleep Apnea: More than 30 events per hour.
- Normal: Less than 5 events per hour.
- Mild Sleep Apnea: 5 to 15 events per hour.
- Moderate Sleep Apnea: 15 to 30 events per hour.
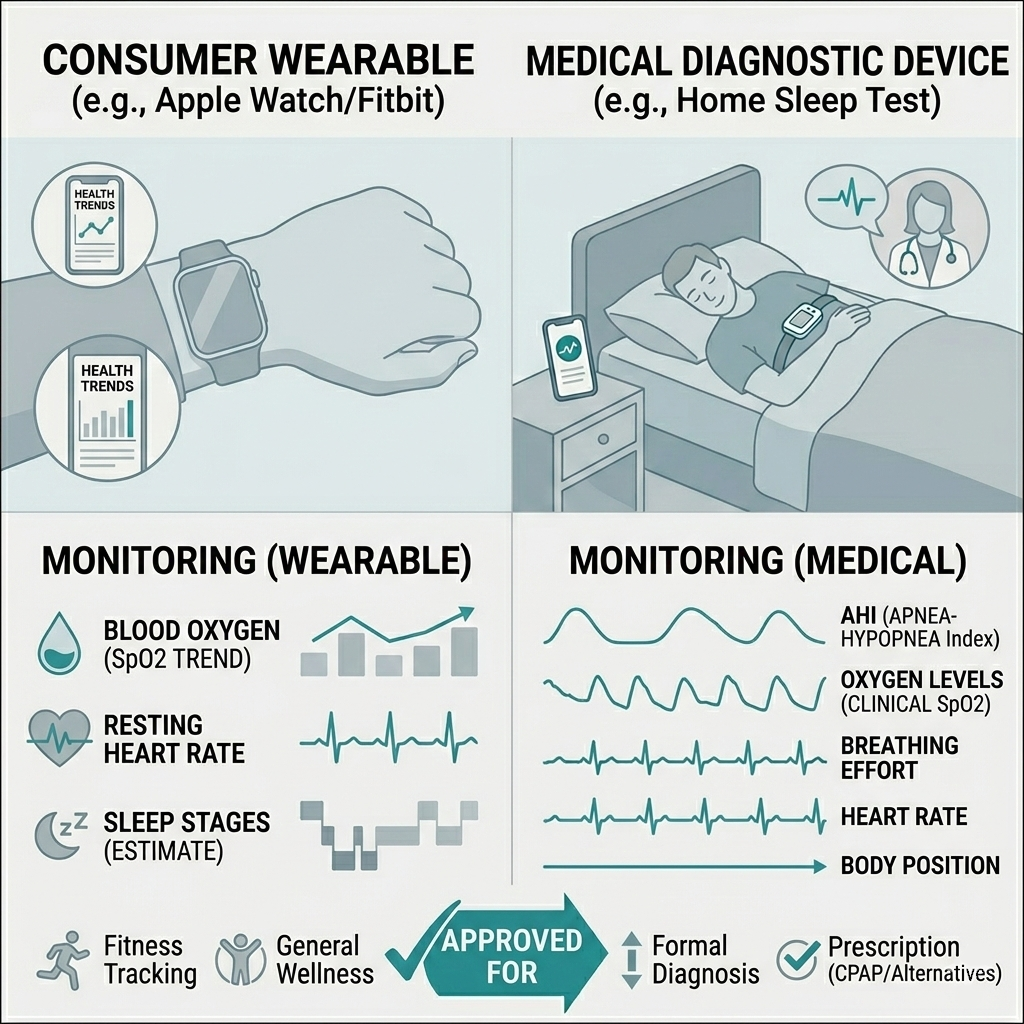
Can I use my Apple Watch or Fitbit to diagnose sleep apnea?
While wearable devices have become excellent at tracking “trends”—such as drops in blood oxygen (SpO2) or high resting heart rates—they are not clinical diagnostic tools.
Think of a wearable like a “smoke detector”: it can tell you there might be a problem, but it cannot tell you where the fire is or how to put it out. To get a prescription for treatment (like a CPAP), you must use a medical-grade device that is reviewed by a licensed physician.
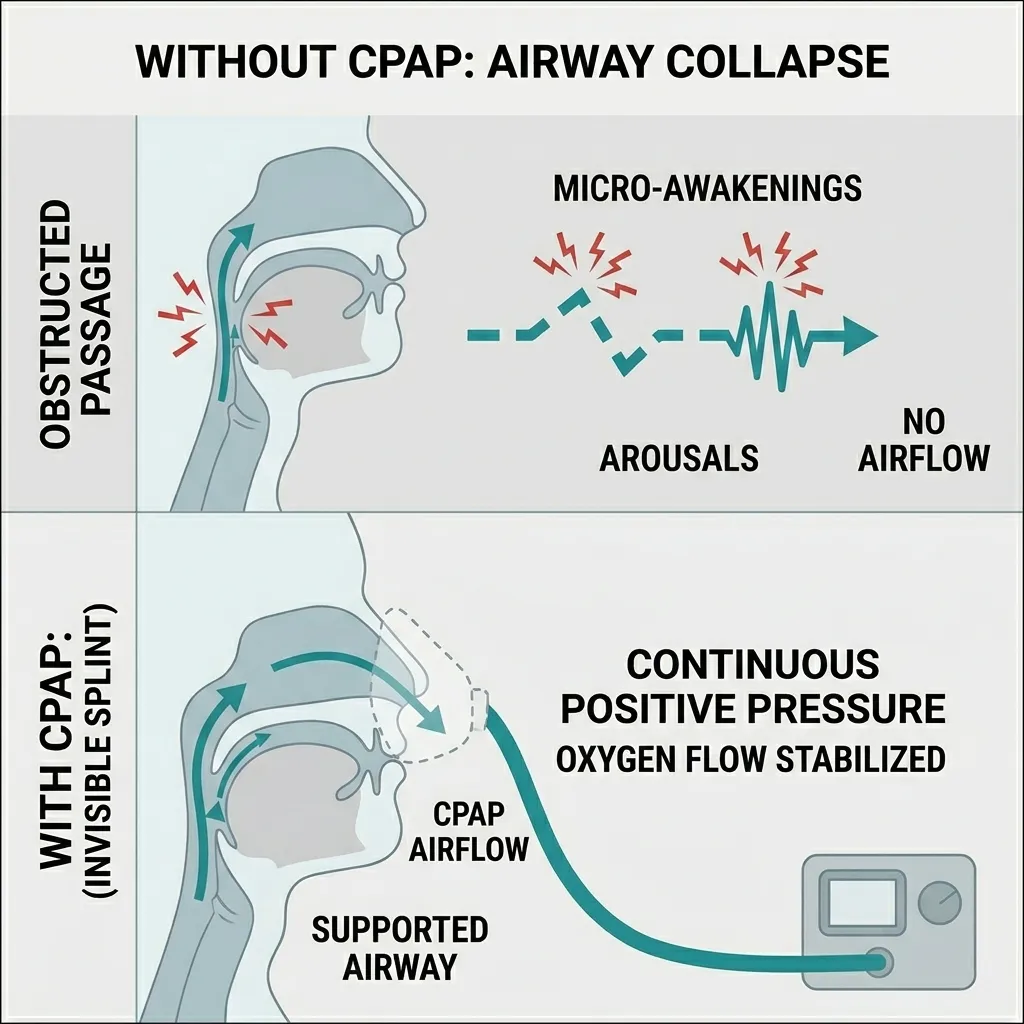
What is CPAP therapy?
CPAP (Continuous Positive Airway Pressure) is the “gold standard” treatment for Obstructive Sleep Apnea.
A CPAP machine works by providing a gentle, steady stream of pressurized air through a mask while you sleep. This air acts as an “invisible splint,” physically holding your airway open so it cannot collapse. By preventing the obstruction, it eliminates snoring, prevents oxygen drops, and allows you to reach the deep, restorative stages of sleep.
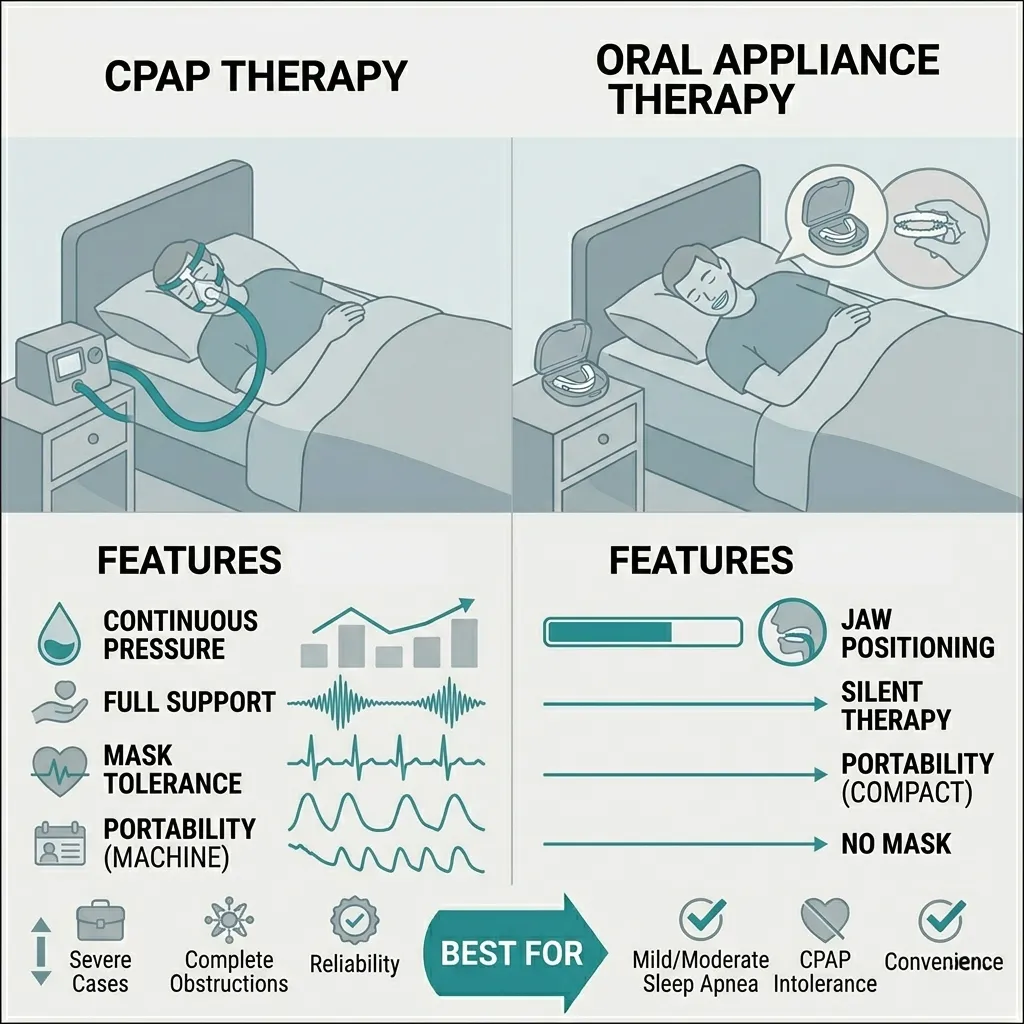
Are there alternatives to CPAP?
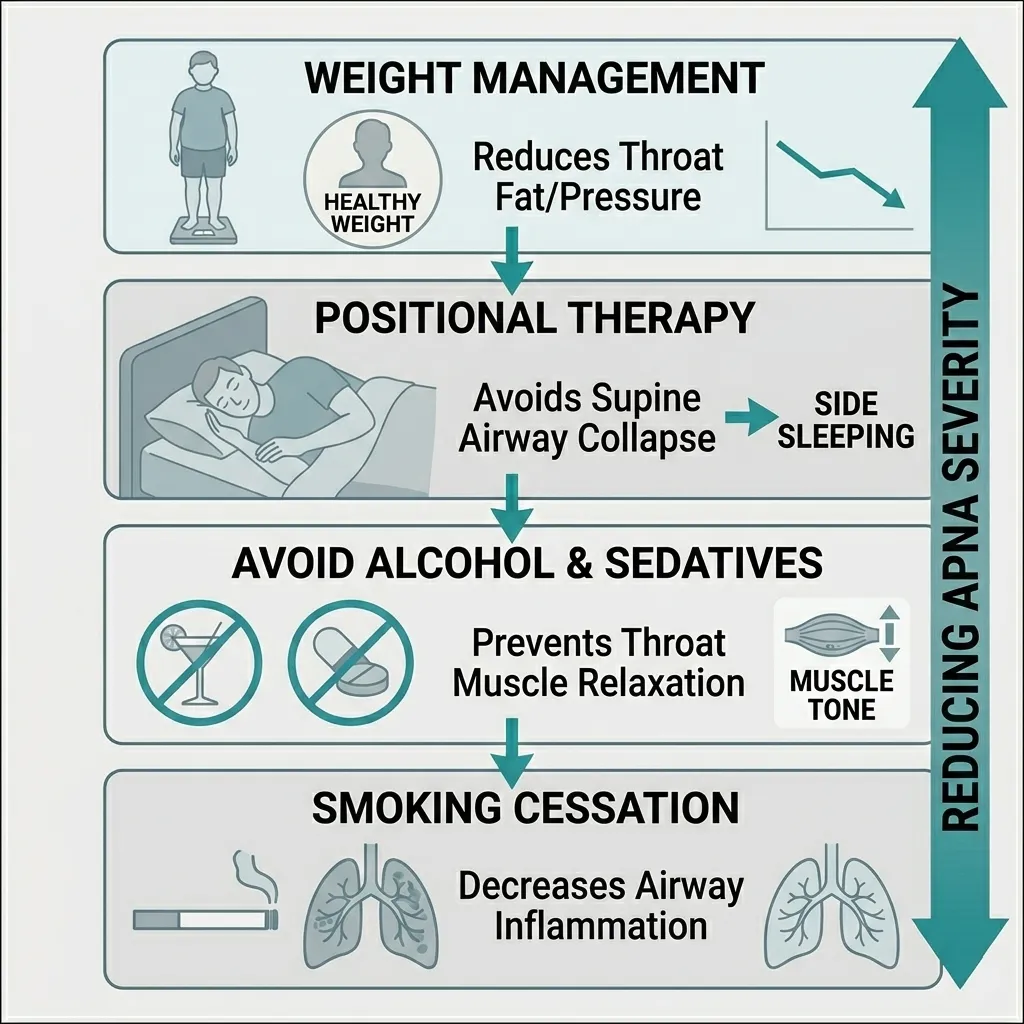
Yes. While CPAP is highly effective, some people find it difficult to tolerate. Depending on the severity of your apnea, other options include:
Surgery: In cases where physical abnormalities (like large tonsils or a deviated septum) are the cause, surgical intervention may be an option.
Oral Appliances (MADs): Custom-fitted dental devices that look like a sports mouthguard. They work by gently pulling your lower jaw forward to keep the airway open.
Positional Therapy: Some people only have apnea when sleeping on their back. Specialized pillows or devices can help train you to sleep on your side.
Lifestyle Changes: Weight loss, reducing alcohol consumption (which relaxes throat muscles), and quitting smoking can significantly reduce apnea severity.
Will I have to wear a mask forever?
Not necessarily. For many, sleep apnea is a chronic condition that requires long-term management, much like wearing glasses for vision.
However, if your apnea is primarily driven by weight or specific lifestyle factors, reversing the condition is possible. If a patient loses significant weight or undergoes successful corrective surgery, their AHI score may drop into the “Normal” range, allowing them to discontinue therapy after a follow-up sleep study confirms the change.